The ambient scribe was supposed to be the revolution. And it was — for documentation. Heidi, TORTUS, Abridge, Freed, Nuance DAX: these tools listen to consultations and generate clinical notes, saving clinicians hours of after-hours paperwork. NHS England's evaluation suggests two to three minutes saved per consultation. Multiply that across a full clinic day and you recover meaningful time.
But documentation is only one segment of the clinical workflow. Before the patient walks in, someone has to review the chart, reconcile recent investigations, check what happened at the last appointment, and identify care gaps. After the patient leaves, someone has to code the encounter, generate referral letters, create patient-facing summaries, initiate prior authorisation, and schedule follow-up. And increasingly, someone has to contact the patient to confirm attendance, gather pre-visit information, and check outcomes days later.
Today, "someone" is a combination of receptionists, medical assistants, nurses, practice managers, and the clinician themselves. Tomorrow, "someone" may be a single AI agent that handles the entire loop — from the first phone call to the follow-up check.
This is not speculation. The pieces are already being built. They just have not been connected yet.
What the Full-Loop Agent Looks Like
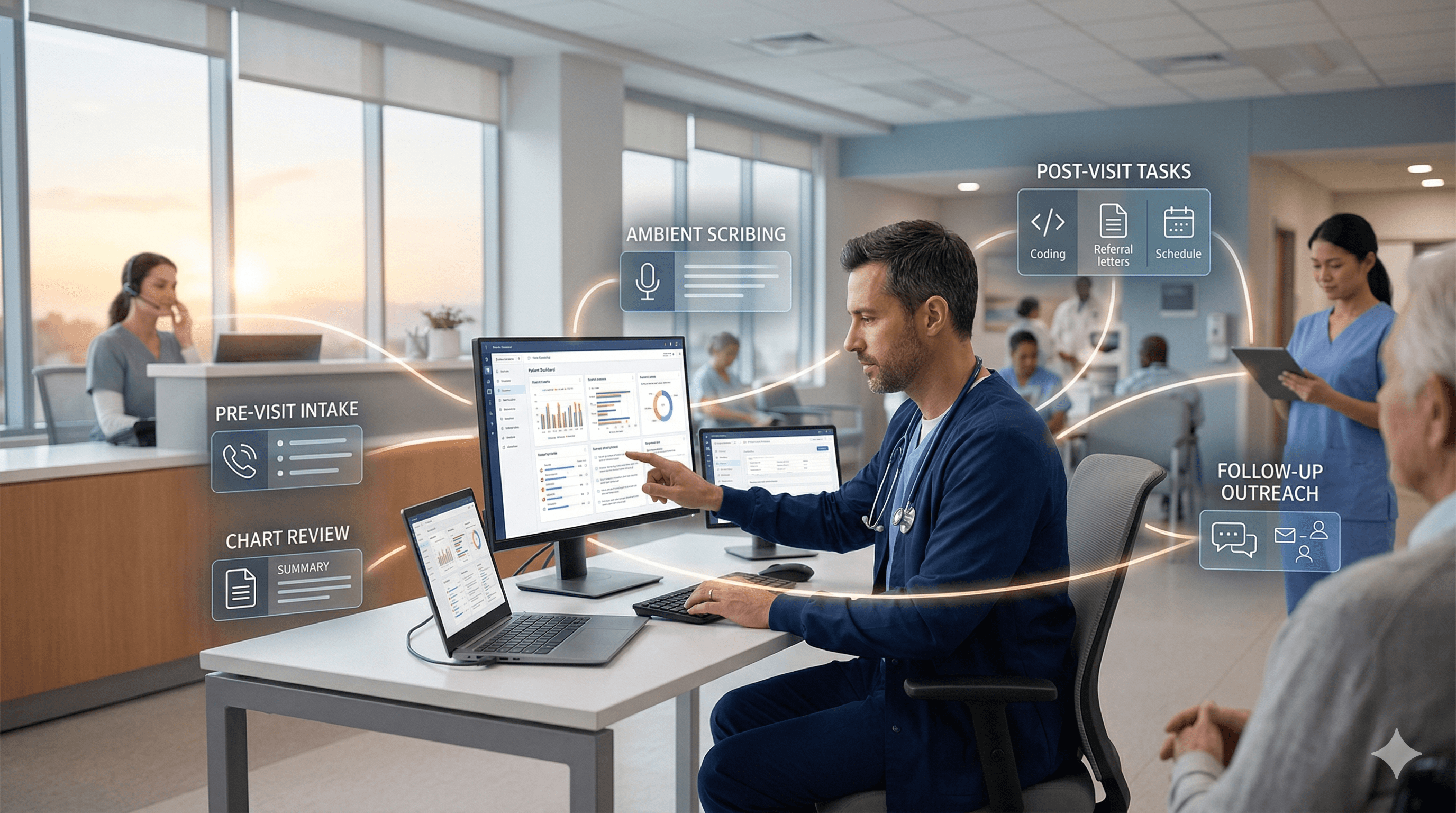
A fully realised clinical AI agent would operate across six stages of every patient encounter.
Stage 1: Pre-visit outreach. The AI agent contacts the patient 24-48 hours before their appointment via phone call, text, or app message. It confirms attendance, gathers updated symptom information, asks about medication changes, collects structured intake data, and flags any urgency that might require rescheduling or escalation. This is not an automated reminder — it is a conversational intake that replaces the clipboard in the waiting room.
Stage 2: Pre-charting. The agent takes the information it gathered from the patient, combines it with EHR data — past consultation notes, recent lab results, imaging reports, discharge summaries, specialist letters, medication lists — and generates a structured clinical brief. The clinician reviews a concise, problem-oriented summary rather than clicking through dozens of EHR tabs. An AAFP study with Navina, the leading pre-charting platform, showed a 61% reduction in visit preparation time and a 25% increase in diagnoses identified.
Stage 3: Real-time documentation. During the consultation, the agent listens ambientally and generates structured clinical notes in real time — the functionality that current scribes like Abridge, Freed, and Nuance DAX already provide. But because the agent prepared the pre-chart, it has context: it can distinguish between information discussed for the first time and information that was already known, flag discrepancies between what the patient reported in the pre-call and what they say in the room, and auto-populate relevant history.
Stage 4: Real-time clinical support. During the consultation, the agent surfaces relevant clinical guidelines, flags drug interactions based on the medication list it has already reviewed, and suggests investigations or referrals consistent with the clinical picture. This is where the knowledge layer integrates. A tool like iatroX — grounded in NICE, CKS, SIGN, and SmPC/emc guidelines — provides the citation-first clinical reference that the agent draws on for guideline-linked recommendations. The clinician sees the evidence, verifies the source, and makes the decision.
Stage 5: Post-visit execution. The agent generates the finalised clinical note, suggests appropriate clinical codes, drafts referral letters, creates a patient-facing summary in plain language, initiates prior authorisation where needed, and schedules follow-up actions.
Stage 6: Follow-up outreach. Days after the visit, the agent contacts the patient to check outcomes: did the symptoms improve? Were the medications tolerated? Did they attend the referral? Did they understand their care plan? The answers feed back into the chart for the next pre-chart cycle.
This is a closed loop. The AI is present at every stage, accumulating context as it goes. Each stage makes the next stage better because the agent carries forward everything it has learned.
Who Is Building Toward This
No single vendor has built the complete loop yet. But several are assembling large sections of it.
Navina owns pre-charting. It is the category leader, with back-to-back Best in KLAS awards for Clinician Digital Workflow. The AAFP-validated platform reconciles data from EHRs, health information exchanges, claims, and unstructured notes into a unified patient summary. It also surfaces HCC coding gaps and care gap closures at the point of care. US primary care focused.
DeepScribe has an explicit AI Pre-Charting product alongside its ambient scribe, pulling clinical details from the EHR and outside sources. It claims to cut pre-visit charting to three minutes. Strong in oncology.
Abridge is expanding from ambient scribe into pre-charting (inpatient workflow), post-visit (prior authorisation via Availity, patient after-visit summaries), and order suggestions. Enterprise, Epic-embedded. Won Best in KLAS for Ambient AI two consecutive years.
Freed has added pre-visit summaries ("chat with Freed to dig into patient note history") and post-visit patient instructions, ICD-10 coding, and clinical letters. Accessible to small practices.
Nuance/Microsoft Dragon Copilot is the platform with the broadest ambition. DAX handles ambient documentation. Dragon Medical One handles dictation. The Desktop Copilot works across apps and EHRs. Nursing documentation launched in 2026. Order suggestions from ambient recordings are live. Microsoft has the Azure infrastructure, the Epic partnerships, and the Teams/phone integration to build the full agentic loop. Available in the US, Canada, and the UK.
DeepCura is closest to the complete loop for small practices: AI receptionist answering calls plus ambient scribe plus billing validation plus fax processing plus EHR write-back, all in a single platform.
In the UK, no vendor has built any portion of this loop beyond ambient scribing. The AI receptionist vendors (QuantumLoop EMMA, InTouchNow) do not connect to scribing. The scribe vendors (Heidi, TORTUS) do not connect to reception or pre-charting. The triage tools (Accurx, eConsult, Anima) do not connect to documentation. The loop is entirely fragmented.
Where the Knowledge Layer Fits
A full-loop agent that prepares, documents, and follows up still needs to make clinically sound recommendations at every stage. When the pre-visit call identifies a symptom that might require escalation, the agent needs to know the escalation criteria. When the pre-chart identifies a medication that interacts with a new prescription, the agent needs current pharmacological guidance. When the post-visit follow-up assesses whether outcomes match expectations, the agent needs guideline-based benchmarks.
This is the knowledge layer — and it is where iatroX fits. A clinical reference platform grounded in NICE, CKS, SIGN, and BNF content, with citation-first answers and direct links to primary sources, provides the evidence foundation that any clinical AI agent needs. Whether that agent is a standalone loop or a collection of integrated tools, the knowledge layer is the component that ensures every AI-generated recommendation is guideline-grounded, verifiable, and current.
Ask iatroX provides rapid guideline retrieval at any stage of the workflow. The Knowledge Centre provides structured access to national guidance. The Brainstorm tool supports clinical reasoning for complex cases. These are not competing with the workflow tools — they are the layer that makes the workflow tools clinically safe.
The Pitfalls
Patient consent at scale. An AI agent that contacts patients, gathers health information, listens to consultations, and follows up afterwards touches patient data at every stage. The consent architecture is far more complex than for a scribe operating within the consultation room alone. In the UK, this crosses GDPR, NHS DSPT, and potentially MHRA territory.
Escalation logic. If the pre-visit agent identifies clinical urgency during the outreach call — chest pain, suicidal ideation, acute deterioration — what does it do? The escalation pathway must be fast, robust, and tested against realistic scenarios.
Context contamination. If the scribe already "knows" what the patient said during the pre-visit call, it may bias the clinician's approach. The pre-chart advantage could become a framing disadvantage if it anchors the clinician on a particular narrative before they have assessed the patient independently.
Liability. If the AI pre-chart omits a critical finding from the record and the clinician misses it, the accountability remains with the clinician — but the risk profile is different because the omission happened before the encounter rather than after.
Workforce displacement. A full-loop agent does not just save clinician time. It potentially replaces receptionists, medical assistants, pre-visit nurses, coders, and follow-up staff. The workforce implications are larger than any single AI category.
The Timeline
The complete loop will not arrive as a single product launch. It will emerge through incremental expansion of existing tools.
In the US, the most advanced players — Navina (pre-chart), Abridge (scribe + post-visit), Nuance (scribe + orders + letters) — will continue expanding along the workflow chain. The first vendor to credibly offer "pre-chart to follow-up" as a unified product will define the category.
In the UK, the loop remains entirely fragmented, and the first vendor to connect even two adjacent steps — reception to scribe, or scribe to coding — will have a significant advantage.
For clinicians, the practical advice is the same regardless of timeline: adopt the tools that solve your most pressing bottleneck today (documentation, pre-charting, or reception), ensure they integrate with your clinical system, and use a reliable knowledge layer like iatroX to verify the clinical recommendations that any AI tool generates.
Conclusion
The full-loop clinical AI agent is the logical endpoint of the ambient scribe revolution. Documentation was the first problem solved. Pre-charting is next. Post-visit execution is expanding. Outreach and follow-up are the final frontier.
The race to build it is already underway. The winners will be the vendors that assemble the most complete workflow, integrate most deeply with EHR systems, and maintain clinical safety across every stage.
The clinician's role does not disappear in this future. It sharpens. When the AI handles the preparation, documentation, coding, and follow-up, the clinician's job becomes what it should always have been: clinical judgement, human connection, and professional accountability — the things that no loop can automate.